Abstract: Fatty liver refers to excessive fat accumulation in the liver, accounting for more than 5% of liver weight. Changes in diet, less exercising and metabolic diseases(e.g. obesity, hypertension, diabetes etc) increase. The incidence of fatty liver disease(FLD) increases annually. FLD has become one of common hepatopathies worldwide. Early symptoms of most patients are not found. Without timely intervention, steatohepatitis, hepatic fibrosis and even cirrhosis may happen. Thus, people should pay more attentions on FLD.
Keywords: Fatty Liver Disease, Causes of Fatty Liver, Fat Accumulation, Targeted Therapy, Metabolic Disorder
1. Type of Fatty Liver Diseases
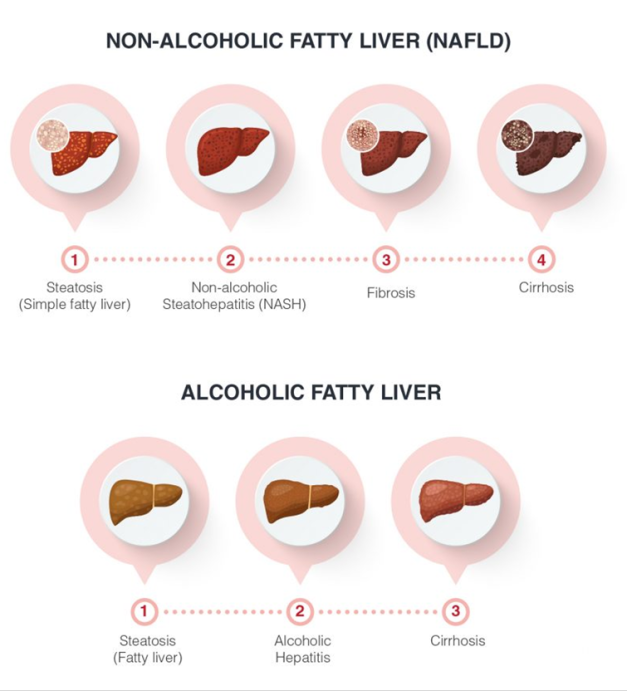
Fatty liver diseases include non-alcoholic and alcoholic liver disease. NAFLD is not relevant to drinking, but often related to metabolic disorders(e.g. obesity, diabetes, hyperlipidemia etc), possibly turning into steatohepatitis or cirrhosis. AFLD is induced by long-term drinking. Alcoholic metabolites can damage hepatocytes, resulting in hepatitis, fibrosis and even cirrhosis further.
2. Causes of Fatty Liver
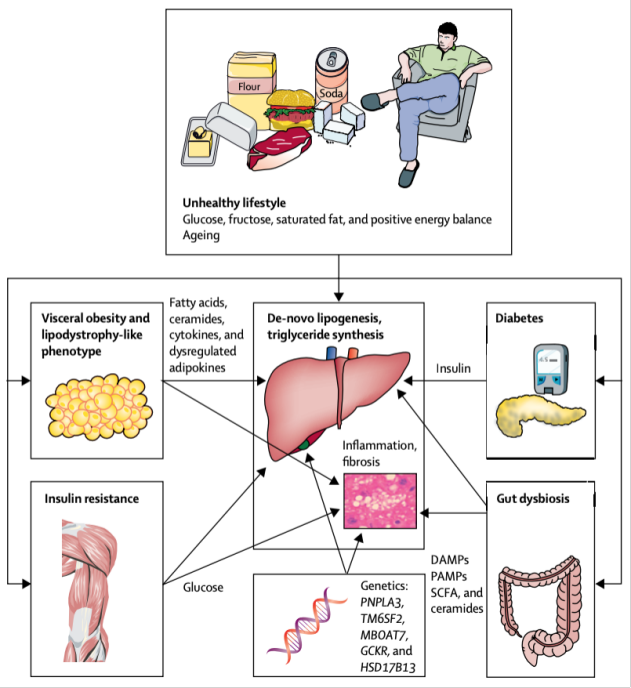
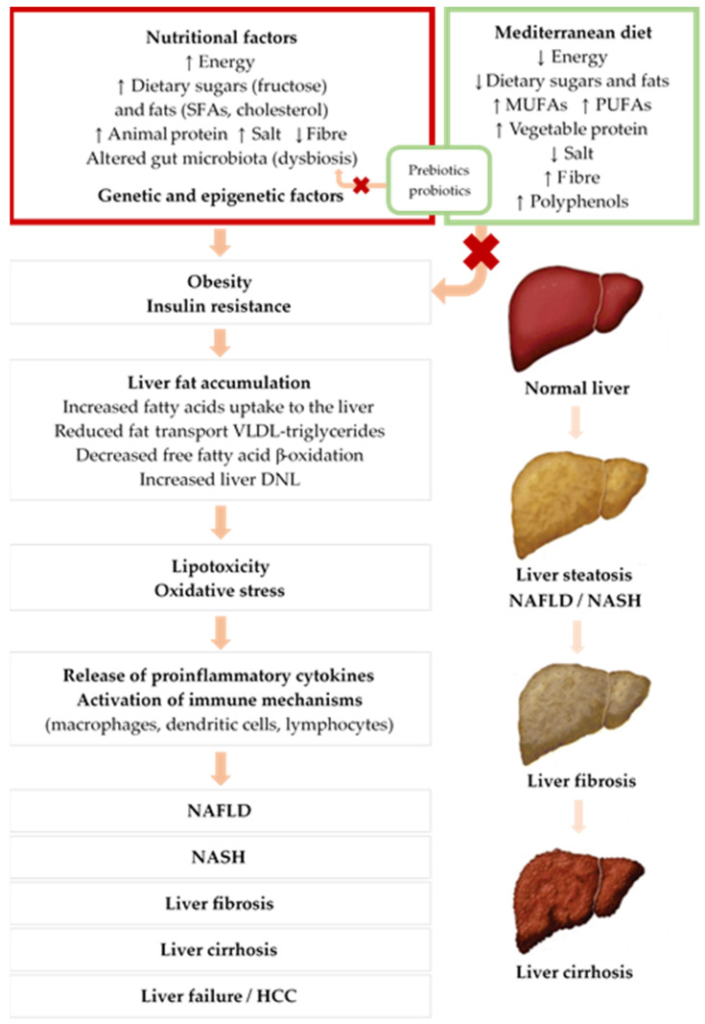
Fatty liver disease is often induced by excessive fat intake, metabolic disorders and decreased fat processing through liver etc. First, insulin resistance is one of the core mechanisms, and often happens among metabolic syndrome patients. Due to decreased insulin effects, accumulation of fatty acid and glucose in vivo promotes fat deposition in the liver. Second, metabolic dysfunction-associated fatty liver can cause delayed steatolysis or energy conversion. Besides, excessive fat deposition in hepatocytes can induce oxidative stress, hepatocyte injury and chronic inflammation, turning into non-alcoholic steatohepatitis(NASH) further. Hepatic fibrosis or cirrhosis may happen. Finally, genetic factors also play an important role in fatty liver disease. Mutation of some genes may affect fat metabolism. Individuals are more easily susceptible to fatty liver.
3. Hazards of Fatty Liver
Early symptoms of fatty liver are not obvious. Delayed intervention may induce various serious complications. First, long-term fat deposition in the liver and inflammatory response can cause hepatic fibrosis and even cirrhosis. Worse still, hepatic failure can be induced. Second, risk of NAFLD or NASH patients obviously increases, especially for those already suffering from fibrosis or cirrhosis. Besides, fatty liver often co-exists with metabolic syndromes(e.g. hypertension, hyperlipemia and diabetes etc). These factors obviously increase the risk of cardiovascular disease. Thus, fatty liver is not just the hepatopathy, but warning for general health.
4. SREBP-targeted Therapy for NAFLD
4.1. Synthesis of Small Molecule Drugs
Fatostatin can inhibit SCAP transport and prevent activation of SREBP. Hep@PGEA carrier delivers MST1 gene. AMPK/SREBP-1c pathway decreases lipid accumulation. 25-hydroxyvitamin D and derivatives KK-052 promote degradation of SCAP, and inhibit activity of SREBP. Decoy oligonucleotides can block transcription; 25-hydroxylanosterol effectively inhibits SREBP pathway and improves NASH via targeting INSIG protein.
4.2. Natural Small Molecule Drugs
Natural substances (e.g. betulin, sulforaphane, isoquercitrin etc) activate AMPK or promote degradation of SREBP via down-regulating expression of SREBP. Regulation of lipid metabolism improves NAFLD.
4.3. Regulation of miRNA
miR-33a, miR-23a/b-3p and miR-615-5p can regulate lipid metabolism via affecting SREBP and target genes, providing novel therapies for NAFLD.
4.4. Other Regulation
MLN4924 decreases hepatic lipid via blocking neddylation. SREBP may negatively regulate hepatic fibrosis, providing new targets for NASH treatment.
5. Prevention and Treatments of Fatty Liver
Fatty liver treatments mainly depend on lifestyle interventions, including:
Diet control: Increase of dietary fiber intake, decrease of high-fat and high-carbohydrate diets
Weight loss: Insist on 150 min of moderate-exercise per week to lose weight and improve insulin resistance. 5-10% decrease of weight helps to reduce hepatic fatty and slow down the development of the disease. Specific drugs are not available. Some patients can try insulin sensitizers. Besides, alcohol and other substances harmful to liver should be avoided.
NAFLD is the metabolic disease affecting various systems. Treatments are involved in liver and multidisciplinary management. As key regulatory factor for lipid synthesis, SREBP has become the important target for new drug development and is expected to promote NAFLD therapy.
6. Recommended Products
| Target | Antibodies | Recombinant Proteins | ELISA Kits |
| ADP | ADP antibody | ADP recombinant protein | ADP ELISA Kit |
| Resistin | Resistin antibody | Resistin recombinant protein | Resistin ELISA Kit |
| Insulin | Insulin antibody | Insulin recombinant protein | Insulin ELISA Kit |
| Hyaluronic Acid | Hyaluronic Acid antibody | Hyaluronic Acid recombinant protein | Hyaluronic Acid ELISA Kit |
| TIMP-1 | TIMP-1 antibody | TIMP-1 recombinant protein | TIMP-1 ELISA Kit |
| MDA | MDA antibody | MDA recombinant protein | MDA ELISA Kit |
| 4-HNE | 4-HNE antibody | 4-HNE recombinant protein | 4-HNE ELISA Kit |
| TNF-α | TNF-α antibody | TNF-α recombinant protein | TNF-α ELISA Kit |
| IL-6 | IL-6 antibody | IL-6 recombinant protein | IL-6 ELISA Kit |
| IL-1β | IL-1β antibody | IL-1β recombinant protein | IL-1β ELISA Kit |
| CRP | CRP antibody | CRP recombinant protein | CRP ELISA Kit |
REFERENCES
[1]Hyperoside modulates bile acid and fatty acid metabolism, presenting a potentially promising treatment for non-alcoholic fatty liver disease, PMID: 40349961.
[2]The association between modified cardiometabolic index with non-alcoholic fatty liver disease and liver fibrosis: a cross-sectional study, PMID: 40247201.