Abstract: Pulmonary hypertension(PAH) is the pulmonary arteriole disease featured with persistent vasoconstriction, thickening and remodeling. The increased pulmonary vascular resistance causes right heart failure and even death. Normal pulmonary artery pressure is lower than systemic circulation pressure. If mPAP in resting conditions is above 25 mmHg, pulmonary hypertension is definitely diagnosed.
Keywords: Pulmonary Hypertension, Increased Blood Pressure, Lung Disorder, Rare Disease
1. Pathology of Pulmonary Hypertension
Pathologic features of PAH mainly include:
- Pulmonary arteriole remodeling: Abnormal proliferation of endothelial cells and smooth muscle cells causes vascular stenosis;
- Vascular endothelial dysfunction: Vasodilatory substances decrease. Vasoconstrictive substances increase;
- Increased pulmonary vascular resistance: Right heart load also increase.
Besides, inflammatory response and fibrosis damages vascular structures further, promoting the development of the disease.
2. Pathogenesis of Pulmonary Hypertension
Pathogenesis of pulmonary hypertension(PAH) is complex, involving various molecular and cellular processes below.
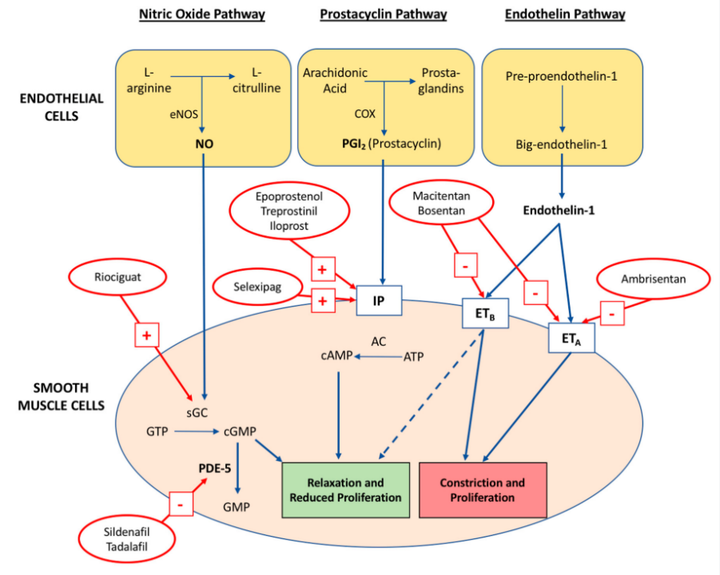
2.1. Endothelial Dysfunction and Imbalanced Vasoconstriction
Pulmonary vascular endothelial cells play an important role in regulating vasomotion. PAH patients always suffer from endothelial dysfunction. Increased vasoconstrictor factor ET-1 and activated ETA/ETB receptor promote contraction and proliferation of smooth muscle cells. Decrease of relaxing factors(e.g. NO, PGI2) is induced by reduced eNOS activity and weakened IP receptor function. Restriction of vasodilation promotes persistent vasoconstriction and remodeling, aggravating the disease further.
2.2. Proliferation of Smooth Muscle Cells and Vascular Remodeling
Conversion of pulmonary artery smooth muscle cells(PASMCs) from low proliferation to abnormal proliferation and anti-apoptosis results in vascular stenosis and increased resistance. Increased calcium signaling promotes persistent smooth muscle contraction. Mitochondrial dysfunction and glycolysis support high cell proliferation. Over-expression of growth factors(e.g. PDGF, TGF-β and FGF) promotes deposition of extracellular matrix and vascular sclerosis.
2.3. Inflammation and Dysimmunity
Researches show PAH patients usually suffer from chronic inflammation. Various inflammatory factors are up-regulated in pulmonary vessels. Pro-inflammatory cytokines(e.g. IL-6, MCP-1) can promote abnormal proliferation of endothelial cells and smooth muscle cells. Besides, the incidence of PAH increases in autoimmune diseases patients(e.g. systemic lupus erythematosus and scleroderma), indicating important roles of dysimmunity in pathogenesis.
2.4. Metabolic Disorder and Oxidative Stress
Metabolic disorder plays a key role in PAH disease, including enhanced glycolysis, lipid metabolism disorder and increased oxidative stress. Activated glycolysis in patients' PASMCs and damaged mitochondrial function show high proliferation. Decrease of PPARγ function results in lipid metabolism disorder, and promotes vascular remodeling. Besides, reduced SOD activity accumulates ROS, damages endothelium and accelerates proliferation of smooth muscle cells.

3. Pulmonary Hypertension Clinical Manifestations
Causes of pulmonary hypertension(PAH) are occult. Early symptoms are not obvious, and usually misdiagnosed as other cardiopulmonary diseases. Early symptoms are shortness of breath during exercise. With the development of the disease, dyspnea in resting conditions also appears. Some patients may also suffer from cough, hemoptysis or hoarseness. Cardiovascular symptoms include chest pain, palpitation, fatigue, dizziness. Fainting may happen in severe patients. Right heart failure may appear in the advanced phase, manifesting as venous engorgement in the neck, hepatomegaly, ascites and limbs edema. Chronic hypoxia can also cause cyanosis and clubbing digits. Autoimmune diseases or genetic factors exist in some patients, manifesting as systemic symptoms. Early recognition and intervention are very important for prognosis.
4. Pulmonary Hypertension Treatment
Pulmonary hypertension treatments include general nursing, drug and operation. It's suggested to avoid strenuous exercise, low-salt diet and long-term oxygen absorption during general nursing. Calcium channel blockers(e.g. nifedipine, amlodipine) are suitable for patients with a positive vasodilation test. Endothelin receptor antagonists(e.g. Bosentan, Ambrisentan), phosphodiesterase-5 inhibitors(e.g. Sildenafil, Tadalafil) and prostacyclin drugs(e.g. epoprostenol, treprostinil) are effective on vasodilation and decrease of pulmonary artery pressure. Severe patients can consider lung transplantation or atrial septostomy.

Pulmonary hypertension(PAH) is the rare and critical pulmonary vascular disease, often misdiagnosed as asthma or heart disease. Deeper investigation on symptoms, causes and treatment can help early detection and timely treatment, obviously improving patients’ quality of life. PAH patients can benefit a lot from innovative drugs and treatments derived from medical achievements.
5. Recommended Products
| Target | Antibodies | Recombinant Proteins | ELISA Kits |
| IL-1β | IL-1β antibody | IL-1β recombinant protein | IL-1β ELISA Kit |
| ET-1 | ET-1 antibody | ET-1 recombinant protein | ET-1 ELISA Kit |
| ANG II | ANG II antibody | ANG II recombinant protein | ANG II ELISA Kit |
| TGF-β | TGF-β antibody | TGF-β recombinant protein | TGF-β ELISA Kit |
| MMP-2 | MMP-2 antibody | MMP-2 recombinant protein | MMP-2 ELISA Kit |
| MMP-9 | MMP-9 antibody | MMP-9 recombinant protein | MMP-9 ELISA Kit |
| TNF-α | TNF-α antibody | TNF-α recombinant protein | TNF-α ELISA Kit |
| IL-6 | IL-6 antibody | IL-6 recombinant protein | IL-6 ELISA Kit |
| PDGF | PDGF antibody | PDGF recombinant protein | PDGF ELISA Kit |
| VEGF | VEGF antibody | VEGF recombinant protein | VEGF ELISA Kit |
| NT-proBNP | NT-proBNP antibody | NT-proBNP recombinant protein | NT-proBNP ELISA Kit |
REFERENCES
[1]Endothelial SMAD4 Deficiency Promotes Pulmonary Hypertension by Impairing Cell Adhesion and Extracellular Matrix Organization, PMID: 40211949.
[2]Neutrophil-Endothelium Interaction Mediated by S100A9 Promotes Pulmonary Vascular Remodeling During Pulmonary Hypertension, PMID: 40492585.