Abstract: Programmed cell death-1(PD-1) and its ligand 1(PD-L1) are important immune checkpoints regulating adaptive immune response. PD-1 consists of 288 amino acids and is mainly expressed in activated T cell, B cell and tumor infiltrating lymphocyte. PD-L1 consists of 290 amino acids and is widely distributed in tumor and antigen presenting cells. They interact with each other to promote immune escape via inhibiting activity of effector T cell. Anti PD-1/PD-L1 antibody has been applied in obviously improving immunity against tumor, and is the important cancer treatment strategy. Role of PD-1 and PD-L1 in cancer is specified below.
Keywords: PD-1 and PD-L1, Immunity, Cancer Treatment, Autoimmune Diseases, Combination Therapy
1. PD-1 and PD-L1 Mechanism
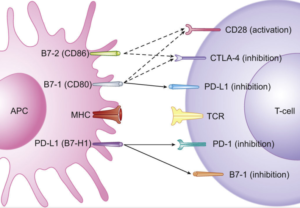
In normal situation, immune system of human body is capable of immunosurveillance. When malignant cells appears, T cell can recognize and kill tumor to inhibit the growth. The activation of T cell depends on dual signals: The first signal is the binding between antigen presented by major histocompatibility complex(MHC) and T cell receptor(TCR). The second signal is effects of co-stimulation and co-suppression.
After PD-1 in T cell binds with PD-L1 in tumor cell or antigen presenting cell(APC), ITIMs and ITSM of PD-1 are phosphorylated to recruit and activate SHP-2. This process effectively inhibits activation of T cell, possibly leading to T cell apoptosis, reduced cytokines, T cell lysis and antigen tolerance. Thus, tumor escapes from immunosurveillance. PD-1/PD-L1 inhibitor prevents the interaction to recover recognition and killing functions of immunocyte, decreasing immune escape of tumor cells.
2. Role of PD-1/PD-L1 in Transplantation and Autoimmune Diseases
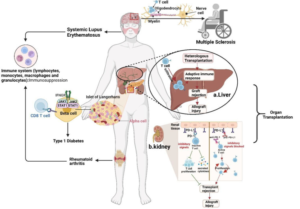
High expression of PD-1 in organ transplantation is on the surface of infiltrative T cell in the grafts. PD-1/PD-L1 mediated negative signal can inhibit over-activation of T cell and induce immune tolerance to decrease immune rejection reaction between host and donor. Blocking the signaling pathway can promote proliferation of infiltrative T cell and exacerbate immune rejection reaction, resulting in severe tissue damage. Besides, dysregulated balance of PD-1/PD-L1 signaling is also related to various autoimmune diseases, e.g. type 1 diabetes, multiple sclerosis, systemic lupus erythematosus and rheumatoid arthritis.
3. Regulation of PD-1/PD-L1 Signalling to Immunocyte
PD-1/PD-L1 pathway promotes depletion and apoptosis of effector T cell, showing increased expression of highly inhibitory receptors(e.g. PD-1, LAG3 and TIGIT), decreased cytokines, and damaged metabolism and proliferation capability. Besides, PD-1/PD-L1 promotes the production of inducible Treg(iTregs) to improve immunosuppressive function via decreasing phosphorylation of PI3K/Akt/mTOR and S6. Besides, this pathway polarizes tumor-associated macrophage to m2 phenotype, promotes angiogenesis and support immune escape of cancer cells. PD-1 and PD-L1 inhibitors can reactivate the anti-tumor response of these immunocytes.

4. Small Molecular Inhibitors Based on PD-1/PD-L1 Signalling Pathway
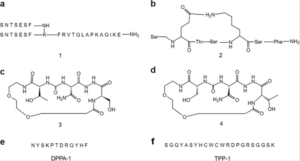
Antibody drugs are featured with poor oral bioavailability, long residece time in tissues and half life, expensive price, inconvenient storage and transportation. These factors restrict clinical applications of PD-1/PD-L1 antibody drugs. Small molecular inhibitors are more suitable for oral administration. Target occupancy can be reduced via regulating half life, thus decreasing the risk of serious immune-related adverse events. In peptidyl small molecular inhibitors, AUNP-12 is the branched chain peptide consisting of 29 amino acids, and sequence can be reconstructed relevantly to extracellular binding domain of human PD-1 protein. DPPA-1 consists of 12 amino acids, specifically affinitive with PD-L1; TPP-1 polypeptide consists of 22 amino acids. Kd for binding with PD-L1 is 74 nmol/L.
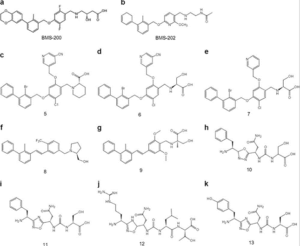
For non-peptide small-molecule inhibitors, scientists have developed a series of biphenyl derivatives, which can overcome antagonistic effects via blocking the interaction between PD-1/PD-L1.
5. Combination Therapy of PD-1/PD-L1 Inhibitors
To overcome the hyporesponsiveness of PD-1/PD-L1 inhibitors, using with anti-tumor drugs targeting different pathways is effective. Immunogenicity of tumor microenvironment is improved. Combination therapy includes cytotoxic chemotherapy and radiotherapy(e.g. CTLA-4, VEGF/VEGFR, MEK, STAT3), decreasing tumor immune escape. Usually, combination therapy is safer than monotherapy. Adverse events don't easily happen. Thus, combination strategy for blocking PD-L1/PD-1 is the research focus in the future.
6. Recommended Products
| Recommended Proteins | |||
| Cat.No | Product Name | Host | Mol. Weight |
| Pr22777 | Recombinant Mouse PD-1 | Mammalian Cells | 58-85 kDa |
| Pr22778 | Recombinant Mouse PD-1 | Mammalian Cells | 33-40 kDa |
| Pr22242 | Recombinant Rat PD-L1 | Mammalian Cells | 40-60 kDa |
| P4902 | Recombinant Human CD247 | E.Coli | 11.2 kDa |
| Recommended Antibodies | ||
| Cat.No | Product Name | Clonality |
| FNab06234 | PD-1 antibody | polyclonal |
| FNab06235 | PD-1 antibody | monoclonal |
| FNab06280 | CD274 antibody | polyclonal |
| FNab06281 | CD274 antibody | monoclonal |
| FITC-30030 | FITC Anti-Mouse CD274(10F.9G2) | monoclonal |
| PE-30030 | PE Anti-Mouse CD274(10F.9G2) | monoclonal |
| APC-30030 | APC Anti-Mouse CD274(10F.9G2) | monoclonal |
| FITC-30044 | FITC Anti-Human CD274(29E.2A3) | monoclonal |
| PE-30044 | PE Anti-Human CD274(29E.2A3) | monoclonal |
| APC-30044 | APC Anti-Human CD274(29E.2A3) | monoclonal |
REFERENCES
[1] ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: a systematic review-based approach, PMID: 31056702.
[2] The Gut Microbiome Is Associated with Clinical Response to Anti-PD-1/PD-L1 Immunotherapy in Gastrointestinal Cancer, PMID: 32855157.