Abstract: Sjögren's syndrome is the chronic autoimmune disease, including symptoms like xeroderma, xerophthalmia and xerostomia etc induced by abnormal attack from immune system. Severe cases can affect visceral organs and result in multiple system damage. This disease can occur irrelevantly, also secondary to autoimmune diseases like rheumatoid arthritis, systemic lupus erythematosus etc. Various clinical manifestations require for comprehensive treatments.
Keywords: Sjögren's Syndrome, Autoimmune Disease, Targeted Therapy, Immune Response, Drug Effects
1. Symptoms of Sjögren's Syndrome
Main syndromes are xeroderma and xerophthalmia, e.g. foreign body sensation in the eye, crying without tears, frequently drinking during speaking. Dry cough or interstitial lung disease affects lung. The kidney may produce proteinuria. Hepatic insufficiency may happen. Decrease of white blood cells or platelet in blood system may appear. Numbness of the extremities and myasthenia may appear in nervous system. Also be aware of systemic adverse effects like painful swelling of joint and palpable purpura on the lower limbs.
2. Causes of Sjögren's Syndrome
Causes of sjögren's syndrome have not been completely determined, induced by genetic and environmental factors. The risk of people with family history of autoimmune diseases and specific genovariation is high. Environmental factors may induce abnormal immune response, e.g. EB virus, hepatitis C virus infection. Besides, incidence rate of female is higher than male, showing possible role of estrogen in the disease.
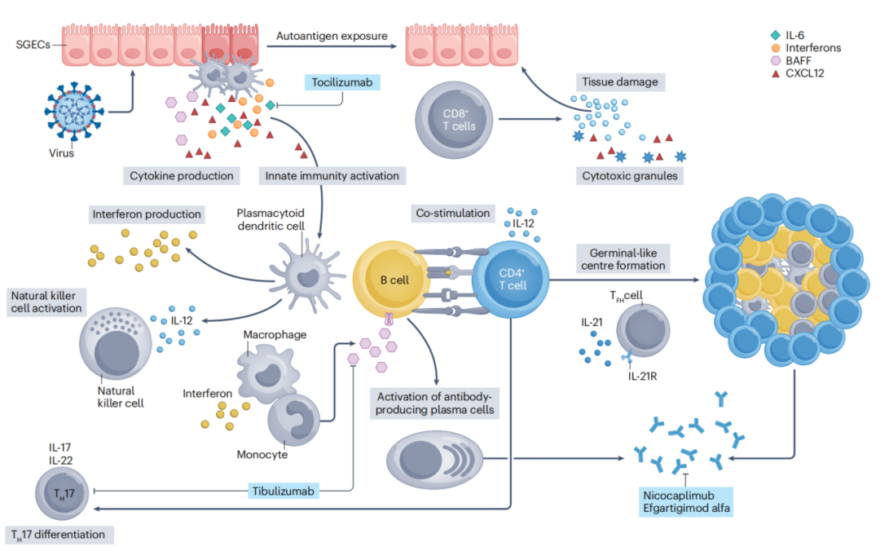
3. Pathogenesis of Sjögren's Syndrome
This disease is first environmentally induced by stimulation of genetically susceptible individuals(e.g. viral infection). Activated SGECs(salivary gland epithelial cells) cause innate immune response. Release of cytokines(e.g. type I interferon, BAFF, IL-6) forms pro-inflammatory environment. pDCs(plasmacytoid dendritic cells) produce a large amount of type I interferon, forming interferon characteristics to accelerate immune activation via JAK-STAT pathway. Monocytes, macrophages, and conventional dendritic cells are involved in inflammatory amplification. Secreted IL-12 and IL-23 promote differentiation of TH1 and TH17. During maintenance of the disease, IL-21 secreted by TFH cell promotes activation of B cell, formation of germinal center-like structures and production of autoantibody. Meanwhile, BAFF supports survival of B cell and increases the risk of lymphoma. Imbalance of TH17/Treg accelerates tissue injury. IL-17 and IL-22 promote the release of chemokine. Manipulating aggregation of B cell and chronic inflammation forms continuous immune attack cycle.
4. Traditional Biological Reagents
Traditional treatments for sjögren's syndrome mostly depend on empirical drugs, and difficultly target for key pathogenesis. Researches show over-activation of autoreactive B cell plays an important role in the disease. Biological reagents can accurately take effects on this target. Specific regulation of immune response can effectively inhibit abnormal activation of B cell and reduce attack on tissues(e.g. salivary gland, lacrimal gland). Thus, symptoms are improved for retarding the development of the disease.
5. New Targeted Therapy
Novartis announced human monoclonal antibody Ianalumab(VAY736) successfully achieved primary endpoint in two phase III clinical trials of sjögren's syndrome(NEPTUNUS-1/2). The safety is also better. Targeted drugs for sjögren's syndrome have not been approved worldwide. Current therapy can only relieve symptoms. Ianalumab targets for BAFF-R, and have two mechanisms: First, remove pathogenic B cells via antibody-dependent cell-mediated cytotoxicity(ADCC); Second, block binding of BAFF with BAFF-R and inhibit activation and survival of B cell. This drug is expected to be first approved for the treatment.
Ianalumab’s clinical success in phase III promotes development of similar drugs, e.g. efgartigimod(target for FcRn), abatacept(target for BAFF/APRIL). In the next 2-3 years, new targeted drugs provide accurate treatment and fundamentally control the disease. Popularization of new therapy requires for more time and efforts from doctors and patients.
| Target | Antibodies | Recombinant Proteins | ELISA Kits |
| IL-6 | IL-6 antibody | IL-6 recombinant protein | IL-6 ELISA Kit |
| Anti-SSA/Ro | Anti-SSA/Ro antibody | Anti-SSA/Ro recombinant protein | Anti-SSA/Ro ELISA Kit |
| SPTAN1 | SPTAN1 antibody | SPTAN1 recombinant protein | SPTAN1 ELISA Kit |
| ANA | ANA antibody | ANA recombinant protein | ANA ELISA Kit |
| BAFF | BAFF antibody | BAFF recombinant protein | BAFF ELISA Kit |
| RF-IgG | RF-IgG antibody | RF-IgG recombinant protein | RF-IgG ELISA Kit |
| IgM | IgM antibody | IgM recombinant protein | IgM ELISA Kit |
| IFN-α | IFN-α antibody | IFN-α recombinant protein | IFN-α ELISA Kit |
| IL-17 | IL-17 antibody | IL-17 recombinant protein | IL-17 ELISA Kit |
REFERENCES
[1]Sjögren's syndrome is associated with a reduction in the surface area of the right caudal anterior cingulate gyrus, PMID: 40629343.
[2]CCR1hi/CCL5hi macrophage-mediated CCL5hi T cell chemotaxis in salivary gland aggravates Sjögren's syndrome, PMID: 40582566.